Barium Swallow – Esophagus
The Common Vein Copyright 2008
Joshua Namias MD
Ashley Davidoff MD
Definition
A barium swallow is a diagnostic study that uses a contrast medium to evaluate the structure and real time function of the esophagus.
The patient is given a barium or gastrograffin drink and examined fluoroscopically. The patient swallows the contrast and images are taken of the barium passage from the mouth down the esophagus.
It is usual also to perform a double contrast study. In this study the patient precedes the barium drink with a small cup of an effervescent mixture similar to a bubbly carbonated drink.
Indication
A barium study is often used to assist in the diagnosis of various esophageal pathologies such as rings/strictures, masses/polyps, ulcers, hernias, altered anatomy such as a corkscrew esophagus, and even disorders of swallowing such as aspiration, esophageal spasm and achalasia, Reflux can also be evaluated. When a ruptured esophagus is suspected it is the procedure of choice and should be performed with gastrograffin.
Alternative, or adjunctive tests include upper endoscopy and manometry. Aspiration and reflux are best observed with the barium swallow. Esophageal leaks and identification of foreign bodies are well evaluated by the swallow in emergency situations. It is a good first test in the patient with dysphagia.
Contraindication
Patients who are unable to swallow the barium material or who are high risk for aspiration should not undergo barium radiography.
Advantages
Barium has the advantage of being less invasive than the some of the other modalities. While there are risks, such as aspiration and allergic reactions, it is thought to be a safe and helpful study especially in those patients who may be at higher risk for one of the other test.
Disdvantages
The main disadvantage of barium radiography is the inability to perform therapeutic modalities when abnormal finding are identified.
Aim
The aim of a barium test is to allow for real-time evaluation of the esophageal contour, anatomy, and swallowing function.
Method
Patient Preparation
Patients present to the fluoroscopy suite within the division of radiology in the fasting state.
After the test they should drink large volumes of water to ensure that the barium is assisted in its passage through the gastrointestinal tract.
Equipment
Contrast material and a fluoroscopic x-ray machine are required for proper visualization.
Technique
Patients are asked to drink the barium material while the radiologist obtains images documenting the passage of barium down the esophagus. The thick barium is used in the double contrast study and the thin in the single contrast study. Gastrograffinis used if there is a clinical concern for perforation. When aspiration is at issue, then gastrograffin is contraindicated because its hypertonic nature will cause significant fluid shift into the lungs.
The double contrast is best used for mucosal evaluation. When possible it is performed on all patients. The patient is standing for the examination. The patient first asked to swallow a mixture of effervescent powder (“fizzies”) mixed in 10 mls of water. Carbon dioxide is released and distends the stomach but also refluxes into the esophagus causing it to distend. 4-5 sips of barium is then “gulped” down in attempt to inhibit peristalsis and distend the esophagus. A pefect double contrast study is not achieved in all patients. This study is best used to study the mucosal surface of the esophagus.
The single contrast study is also performed on all patients and is first performed in the upright projection to evaluate the oropharyngeal phase of the swallow. The patient is asked to holds a mouthful of barium until instructed to swallow. The swallow is followed from the back of the mouth, posterior soft palate, through the valleculae, pyriform sinuses and into the proximal esophagus using rapid film technique because the bolus moves so quickly. This is viewed and filmed in two views. The bolus is then tracked through the upper esophagus, mid and distal esophagus using a variety of filming techniques including changing degrees of obliquity, variation in the rapidity of filming and degree of magnification.
The patient is then placed in the prone projection, with left side slightly up and is again asked to swallow the thin barium. The prone view is best for the evaluation of the distal esophagus and GE junction and hence diseases such as hiatus hernia, peptic strictures are best demonstrated. A full column view of the esophagus is often obtained
Throughout the exam attention to the GE junction is paid in order to evaluate for spontaneous reflux.
The patient is then returned to the upright postion and is asked to swallow a 13mm barium pill to determine if there are any significant strictures.
Results
Images are obtained that allow for evaluation of the swallowing pattern based on the flow of barium. Luminal irregularities can be identified such as ulcers, strictures, extrinisic compression.
The fully distended mucosal surface should be smooth featureless. In about 10% of the older population flat lesions representing glycogenic acanthosis may be seen. Distally the z -line representing the squamocolumnar junction is seen as a zigzaggng line at the level of the diaphragm and esophageal hiatus.
The relief view represents the collapsed esophagus and longitudinal foldsare seen extending the entire length of the esophagus.
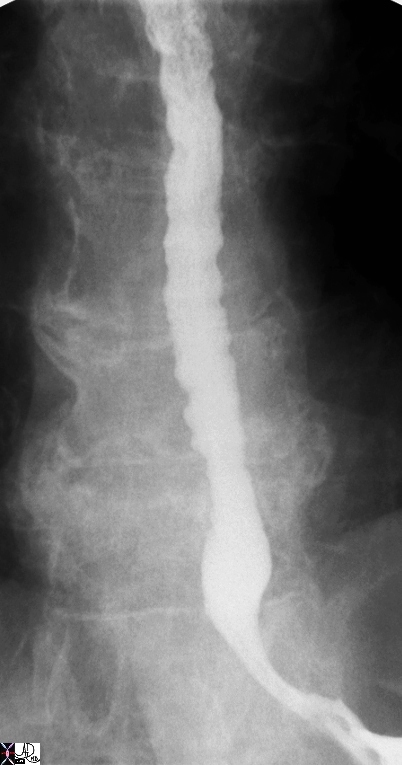
Transverse folds (aka feline esophagus or shivering esophagus ) represent contraction of the longitudinal folds of the musculars mucosa. This finding is seen both in normal patients and in patients wiith reflux.
 Feline Esophagus – Esophageal Shiver Feline Esophagus – Esophageal Shiver |
| 00567b01 esophagus circular folds feline esophagus anatomy normal Courtesy Ashley Davidoff MD |
Two impressions on the esophagus are almost always observed. the first is that of the aortic arch and the second of the left mainstem bronchus. The pulsating impression of the left atrium especially when enlarged can be seen on the lower one third of th esophagus.
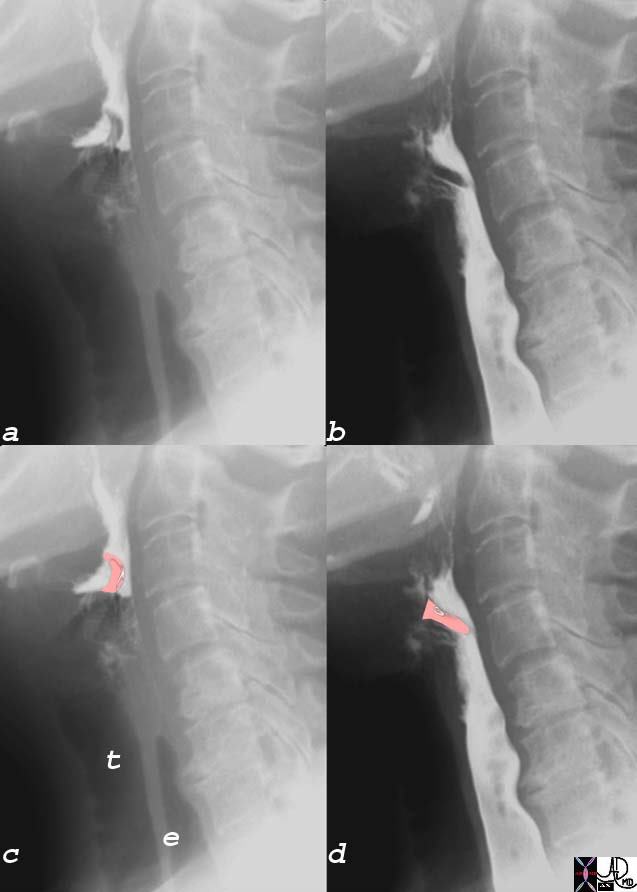 Function of the Epiglottis in Swallowing Function of the Epiglottis in Swallowing |
| 76182c01 epiglottis trachea esophagus osteophytes barium swallow cervical esophagus normal anatomy Courtesy Ashley Davidoff MD |
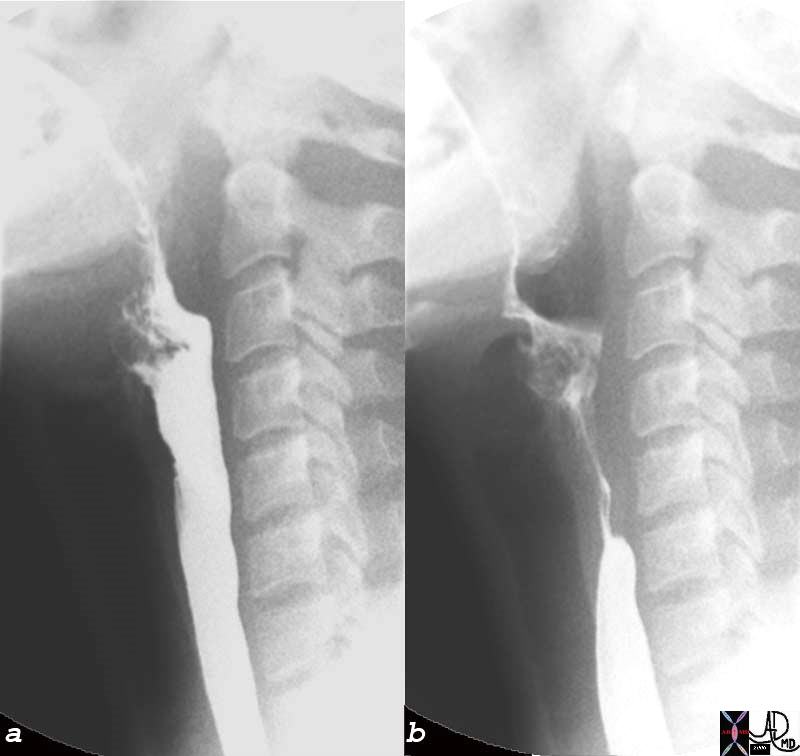 Upper Esophageal Sphincter Open, (a) Closed (b) and beginning of Primary Stripping Wave Upper Esophageal Sphincter Open, (a) Closed (b) and beginning of Primary Stripping Wave |
| 76204c esophagus cervical esophagus UES upper esophageal sphincter beginning of primary stripping wave normal physiology swallowing mechanism function single contrast barium swallow Courtesy Ashley Davidoff MD |
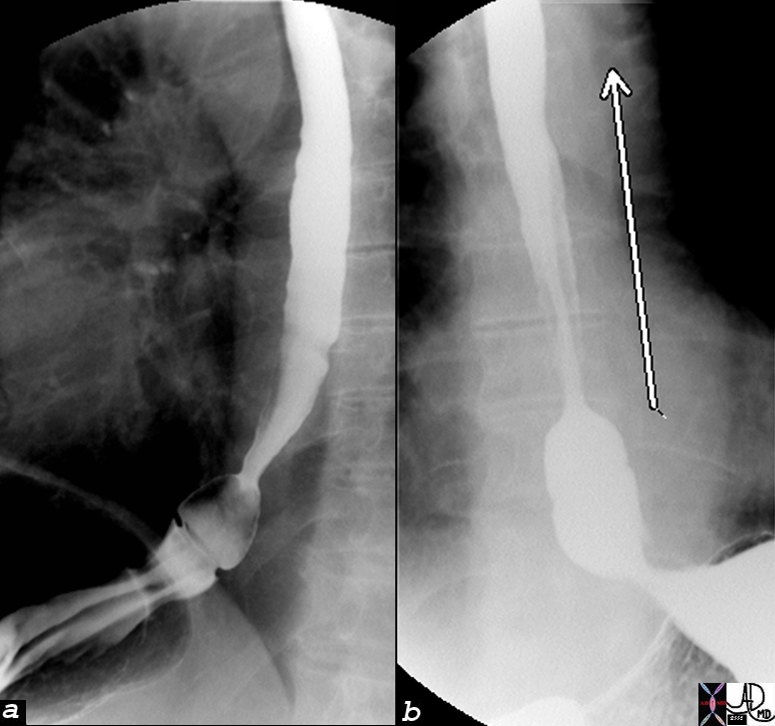
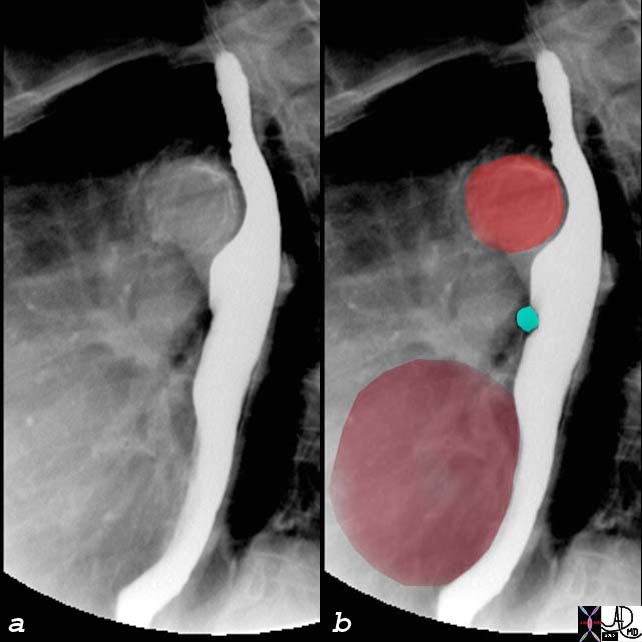 Normal Indentations on the Esophagus Normal Indentations on the Esophagus |
| The normal indentations on the esophagus include the aortic arch and knob seen in bright red in b. The left bronchus is usually seen as a oblique line crossing the back of th esophagus, but in this case is seen as a focal indentation on the anterior wall. The left atrium is seen pulsating against the distal esophagus (maroon) usually when the left atrium is enlarged.
76119c01 esophagus aorta left bronchus left atrium LA normal indentations on the esophagus relations barium swallow Courtesy Ashley Davidoff MD |
Applied Biology
 Tertiary Contraction Waves Tertiary Contraction Waves |
| 76208 esophagus tertiary contraction waves normal function single contrast barium swallow Courtesy Ashley Davidoff MD |


 Esophagitis with Superficial Ulcerations (middle) and Stricture (right) Esophagitis with Superficial Ulcerations (middle) and Stricture (right) |
| Courtesy Ashley Davidoff MD 01221 esophagus + reflux esophagitis stricture ulcer barium swallow upper GI UGI imaging radiology contrast X-Ray |
 Gastroesophageal Reflux Gastroesophageal Reflux |
| 76171c01 esophagus GE junction gastroesophageal junction squamo-columnar junction z line epiphrenic ampulla gasrtric mucosa small hiatus hernia large amount of reflux to thoracic inlet double contrast barium swallow Courtesy Ashley Davidoff MD |
The abnormal esophagus may show nodularity, punctate collections of barium surrounded by a rim of edema, or linear ulcers with surrounding edema. The surface edge of the esophagus should be smooth. Any irregularity usually suggests esophagitis. of the nodular
Complications
Complications related to barium esophography are rare. The main complication patients are informed of is aspiration of the contrast material. In patients with slow gastrointestinal transit, the barium can also solidify and form a bezoar, but this is a rare complication.
Conclusion
A barium swallow offers a safe and effective means of evaluating the structure and function of the esophagus, offering a unique ability to evaluate for aspiration